Corona
virus Vaccine in Development
As
the new coronavirus was becoming a global
pandemic, researchers began working on a vaccine. It’s no quick fix — it
can take up to a year and a half for a vaccine for the virus, which
causes the disease COVID-19, just to move from the lab to human trials.
Unfortunately
even in this advanced technology world we are still unable to manufacture
vaccines of many past epidemic or pandemic disease.( read article of pandemic
disease in history and deadly virus in history to know more about vaccines
which are developed or not developed for the disease yet.)
Currently scientist are
working on making vaccines for corona virus with new technology which is mRNA-based
vaccines that have the ability to elicit potent immune responses against
infectious diseases and certain cancers.
Whereas the Traditional
vaccines stimulate the production of antibodies via challenges with purified
proteins from the pathogens, or by using whole cells (live, attenuated
vaccines) which take years to show up in market. Alternatively, RNA-based
vaccines use mRNA that upon entering cells, are translated to antigenic
molecules that in turn, stimulate the immune system which is more rapid and
less expensive than traditional vaccines, which can be a major advantage in
pandemic situations. Clinical trials for an mRNA-based SARS-CoV-2 vaccine are
currently underway.
Currently,
Around the world, more than 40 teams are working on a vaccine for Covid-19.
We
aim to do that either by making a DNA-based vaccine that contains genes that
produce the virus’ protein, or by making a vaccine that includes a portion of
the actual protein.
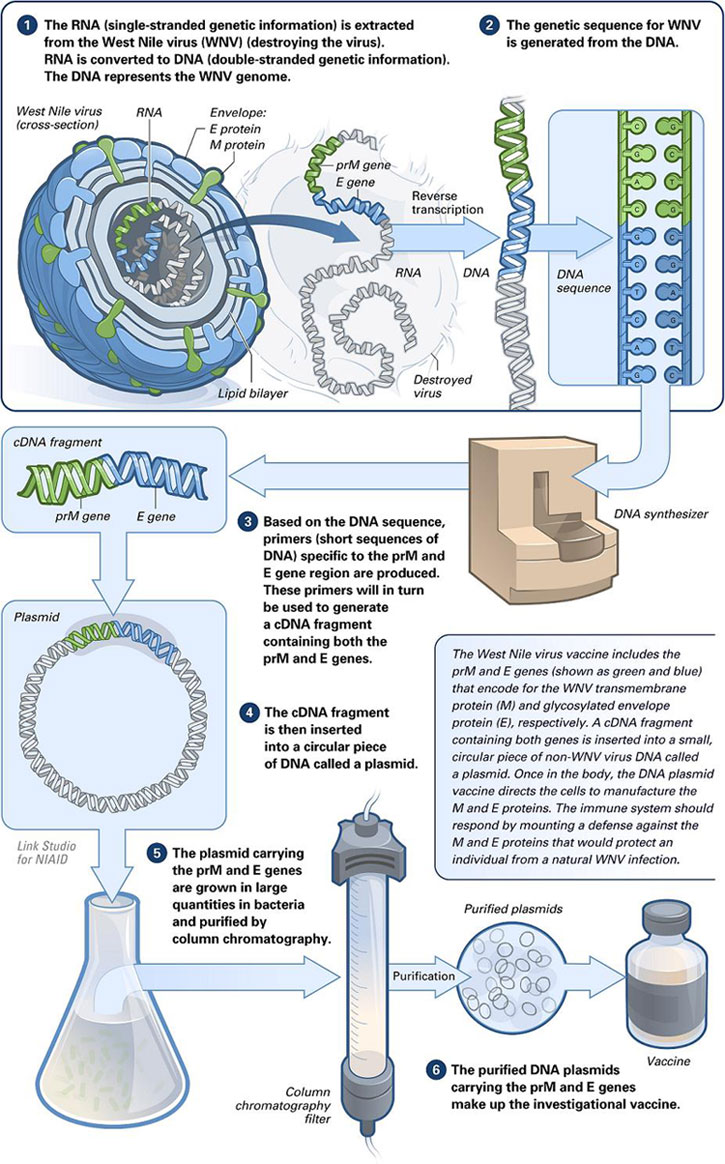
There
are no DNA-based vaccines currently approved for humans, although there is a
West Nile Virus DNA-based vaccine for horses. Protein-based vaccines include
the hepatitis B vaccine.
What are some of the
issues involved in developing this vaccine?
The
major challenge is the speed. Time is of the essence because every moment more
people are getting infected. We can quickly come up with a vaccine in the lab
and test it in animals. But it can take nine months to a year and a half to get
to human clinical trials, which can be very difficult and require a lot of
resources, whether that’s philanthropic or government grants.
Defeating Covid-19 will call for more than vaccines; it will
involve quarantines, social distancing, antivirals and other drugs, and healthcare
for the sick. But the idea of a vaccine – the quintessential silver bullet –
has come to bear an almost unreasonable allure. The coronavirus arrived at a
ripe moment in genetic technology, when the advances of the past half-decade
have made it possible for vaccine projects to explode off the blocks as soon as
a virus is sequenced. These cutting-edge vaccines don’t use weakened forms of
the germ to build our immunity, as all vaccines once did; rather, they contain
short copies of parts of the germ’s genetic code – its DNA or RNA – which can
produce fragments of the germ within our bodies.
Thus, for the first time ever, scientists have been able to
muster up vaccine prospects mere weeks into a new, fast-spreading disease.
Right now, there are at least 43 Covid-19 vaccines in development around the world –
in Brisbane and Hong Kong, in the US and the UK, in the labs of universities
and companies. Most of these are DNA or RNA vaccines. One vaccine, made in 63
days by an American biotech firm named Moderna, moved into human trials on 16
March, entering the bloodstream of the first of 45 healthy adult volunteers in
Seattle. It was a “world indoor record”, said Anthony Fauci, the doctor who
heads the US National Institute of Allergy and Infectious Diseases. “Nothing
has ever gone that fast.”
Until this century, crafting a vaccine for even a long-familiar
pathogen such as the polio virus, ushering it through trials and bringing it to
market could take as long as 10 or 20 years. The first of these three stages is
now staggeringly quick; a scientist at one company, Inovio Pharmaceuticals,
told New Scientist
magazine that her team had a preliminary model for a Covid-19
vaccine after just three hours of work.
The thrust of this revolution – the capacity to create an
infinitesimal part of an already minute virus, without handling a virus
specimen at all – can seem godlike. But the next two stages – testing vaccines
in humans and then manufacturing them for wide use – remain mortally slow. This
is especially so because these newest types of vaccines – DNA or RNA vaccines –
have never yet been licensed for use on humans. Outside a lab, they are
completely unproven. With Covid-19, both contagion and vaccine are so new that
there’s no telling what human trials will reveal, or how long they will take.
Every scientist, policymaker and researcher I spoke to said that we’ll be lucky
to have a vaccine for use within 12-18 months.
If a DNA or RNA vaccine against Covid-19 is ever approved, it
will be a watershed moment – not just because it will bear out the promise of
this technology, but also because the technology will fortify us against future
pandemics. Over the past few years, epidemiologists, risk analysts and
policymakers have made concerted efforts to sharpen research and rethink the
industrial model of vaccine production, all in preparation for the hypothetical
disaster they call Disease X: any unknown disease that springs suddenly into
our species and races ruinously through it. Covid-19 is the first Disease X to
arise since the term was invented, but it won’t be the last. The climate is
warming, we’re hacking down forests, our population is expanding and our skills
at waging biological warfare are improving. The odds that we’ll keep
encountering more and more Disease Xs are increasing. We will need all the
vaccines we can make.
In its essence, even the most advanced vaccine functions on the
same premise as the earliest mode of immunisation: cotton pads soaked in
smallpox pus that were stuffed into the nostrils of healthy children in
16th-century China. The principle of vaccination is still to bluff the body: to
slip in weakened germs, or even parts of germs, that do no harm but induce the
release of antibodies that grant long-lasting immunity. The inducements have
grown more sophisticated, but they continue to rely on the body’s biological
defences. Humankind has developed no system of immune response more effective
than the one that’s been inside us for hundreds of thousands of years.
The latest class of vaccines –hold genetic material such as DNA
or RNA; these are the kind that have never yet been licensed for use. They can
be developed quickly, and they jog our immunity in distinctly different ways
from everything that came before. The oldest method of vaccination involves
dosing a person with inactive or enfeebled forms of the pathogen. For most of
the past century, sourcing these was a laborious affair. For decades,
scientists depleted the strength of viruses by growing them in human cell
strains kept in labs at low temperatures; once the virus was sufficiently weak,
it was safe to be sent into the human body in a vaccine. One line of lung
cells, sourced from an aborted foetus in Sweden and multiplied again and again
in lab cultures in the US, helped inoculate 300 million people against rubella,
rabies, mumps and several other diseases.
In the 1980s, researchers learned to mass-produce sub-units of a
virus, each fragment assembled out of proteins and sugars. This might be a
toxin or a part of the viral shell – just a signature whiff of the pathogen
that can trigger immune reactions when introduced into the body. These molecular
fragments are called antigens, because they generate antibodies that target
them. Despite this technological advance, all these antigens still had to be
cultivated in labs or factories.
It wasn’t until this century that the real leap occurred,
propelling scientists towards DNA and RNA vaccines. Once computers became
powerful enough to sequence the genetic code of a pathogen quickly and cheaply,
scientists were able to easily create snippets of its genes, which could then
be sent into the human body. These snippets, using our own cells as miniature
factories, can manufacture their antigens within us. As soon as a germ’s gene
sequence is known, scientists can begin concocting a vaccine for it.
That’s what happened with Covid-19. On the last day of 2019,
Wuhan’s health authorities reported the strange pneumonia variant to the World
Health Organization. By mid-January, Chinese scientists had posted online the full,
machine-readable genome of the Covid-19 virus: all 29,903 nucleic bases that
comprise its sequence of RNA – ribonucleic acid, its genetic material.
For scientists around the world, this was the starter pistol
being fired. By studying the published genome, they could single out sets of
genes that make specific proteins in the Covid-19 virus: the S-protein making
up the spikes on the virus’s outer envelope, for instance, or the
phosphorus-laden protein in the walls of an inner capsule, packaging the RNA
within.
what
antigens – what portions of the virus – can be found that are similar across a
range of coronaviruses? If scientists discover these and, by deploying them in
vaccines, drill our immune systems to recognise them, we will have given
ourselves a way to fend off several kinds of coronavirus diseases, including
Covid-19. The spike proteins jutting out of all these viruses, giving the
appearance of a fringed crown, are a prime example of such antigens. Every
coronavirus uses its spikes to invade human cells. Once our immune systems
engineer antibodies in reaction to a vaccine of spike-protein antigens, they
will have not just a method to identify coronaviruses, but also a prospective
point of attack to cripple them.
covid antigen attach with human ACE site
Pathology pathway of covid-19
How does this new
coronavirus vaccine compare to other vaccines?
The
new coronavirus continues to evolve, so we need to make sure the portion of the
protein and its genetic sequence we are using to develop our vaccine will still
be effective even if the virus mutates or changes. It’s also possible that the
antibody a vaccine creates could actually make patients more susceptible to the
virus rather than prevent it, so making sure the vaccine targets the right part
of the virus is very important.
How much does it cost to
bring a vaccine to the public?
To
bring a DNA-based vaccine to human trials can cost around $1 million to $2
million, and to bring a protein-based vaccine to human trials can cost around
$1.5 million to $3 million.
Most of this money will go towards trials and production, the
costs of which are now frequently borne by drug companies. After the 80s, when
a series of mergers left the pharma industry in the hands of a few behemoth
companies, vaccines fell thoroughly under the sway of market forces, subject to
the kind of logic that prompted Goldman Sachs, in a 2018 report, to wonder: “Is
curing patients a sustainable business model?” (It isn’t, the analysts concluded.)
Diseases that are borne out of poverty, and that require cheap
vaccines, such as cholera, are largely ignored, says Peter Jay Hotez, the dean
of the National School of Tropical Medicine at the Baylor College of Medicine
in Houston. So are diseases that are uncommon, or diseases that have come and
gone. Taxpayers fund most vaccine research, but the pharma titans that can make
them at scale are reluctant to commit to a vaccine if the likelihood of profit
is meagre. “We have a broken ecosystem for making vaccines,” Hotez told me.
When Sars broke out in 2002, scientists and companies rolled up
their sleeves to deliver a vaccine. But after 2004, no Sars cases were
reported, so research flagged; one vaccine, from Sanofi, never made it past
clinical trials. Ideally, Hotez says, vaccines would still have been run
through the first few steps of trials and kept in reserve for future
emergencies. Between 2011 and 2016, Hotez and his team designed a potential
vaccine for Sars, and had the Walter Reed Army Institute of Research make
20,000 doses, to test on humans. But none of Hotez’s usual funders gave him a
grant for these trials. “Sars dropped off their list of priorities,” Maria Elena
Bottazzi, one of Hotez’s collaborators at Baylor, told me. “We had other
situations, like Ebola or Zika.” The industry’s attention is easily diverted,
Hotez said. “It’s like little kids playing a football game. The ball goes in
one direction and all the kids run after it. Then it goes in another direction
and all the kids run that way.”
So much about Covid-19 is still unclear that companies can’t yet
gauge the profit margins on a vaccine. Will the disease fade before a vaccine
is approved? Will DNA or RNA vaccines even work? Will everyone be inoculated –
a bumper payday from billions of doses – or will vaccines go to just a few
at-risk groups, such as healthcare workers or anyone over 40? “At some point,
there will be a go/no-go decision to make for companies,” said Jason Schwartz,
a vaccine policy scholar at Yale. “And then they’ll have to figure out if it’s
worth the risk.” One way to make it worthwhile is to engage in price gouging,
which drug companies have always been happy to do. Earlier this month, the
US passed a coronavirus
spending bill that deliberately left out controls on vaccine prices.
By the time a vaccine is
ready, will we still need it?
Many
experts suggest that we will. Some predict this will become like the common
cold and disappear in the warmer months and come back in the winter in the
United States. It’s also harder to detect because not all people infected with
the virus have a fever or show other symptoms, and it’s more contagious than
many other viruses, so it likely won’t disappear quickly.
The danger of vaccine
preparation under pressure
The overriding purpose of the process is abundant caution; a
vaccine that unexpectedly proves harmful is the industry’s worst nightmare.
In 1942, a yellow fever vaccine contaminated with a hepatitis B
virus was given to more than 300,000 American troops; nearly 150 of them died.
The field’s classic reference text, Plotkin’s Vaccines, by the physician Stanley
Plotkin, refers sombrely to “the Cutter incident” – a 1955 episode in which a
manufacturer named Cutter Laboratories failed to properly deactivate the virus
in its polio shot. The faulty vaccine caused roughly 40,000 cases of polio,
paralysed 260 people and killed 10.
The US’s strict rules to regulate vaccines emerged, in part, because of
Cutter Laboratories. The company survived, but paid out millions in civil
damages. The Cutter incident set a precedent for more lawsuits during the next
three decades, in which parents argued that their children had been disabled by
malfunctioning vaccines. Some pharma firms, worried about multimillion-dollar
claims settlements, abandoned vaccines altogether; others hiked their prices to
cover any future legal costs. To keep vaccines cheap and vaccinations regular,
the US government had to set up a compensation fund that eased most of the
liability on vaccine companies.
In the midst of a pandemic, so many forces tug at the vaccine
development process – politics, industry, science, money, fear, hope – that
there’s a perpetual hazard of clinical trials being hurried or of a poorly
planned vaccination scheme being rushed out. One historical analogue is found
in 1976 – like 2020, an election year. That February, a bout of swine flu broke
out in an army post in New Jersey, and one soldier died. In comparison to
Covid-19, the outbreak now seems minor, but it jolted President Ford’s
government, which was already suffering from the second-hand shame of Nixon’s
resignation just two years earlier. The administration fretted that, in the
autumn, at the height of flu season, the virus would exact a huge loss of life;
one government estimate figured that 1 million Americans would die.
So Ford announced a plan to vaccinate everyone in the country,
and had the Centers for Disease Control draft a $136m plan to do it. He ignored
Albert Sabin, one of the heroes of the polio vaccine, who advised against
immunisation, believing that no epidemic was imminent. Ford also ignored the
warnings coming out of clinical trials, in which one of the four manufacturers
was found to have formulated some unknown number of its 2.6m doses with a
different flu virus altogether. Congress exempted all these companies from
liabilities if their vaccine harmed anyone. Beginning in October, 40 million
Americans were vaccinated, but by mid-December, it emerged that the shot came
with a slightly increased risk of contracting Guillain–Barré syndrome, an
immobilising neurological condition.
The vaccine campaign was scrapped soon after; by that time,
close to 450 people had been afflicted with Guillain–Barré. It was impossible
to say how many of these cases were seeded by the vaccine. And if the vaccine
really did prevent a swine flu epidemic, there was no way to know; the
counterfactual – no vaccination, a ravaging pandemic – was hidden from view.
This vaccine’s legacy, in public memory, was the paralysis of those hundreds of
people.
Already, the temptation to accelerate the trials of Covid-19
vaccines is becoming apparent. Earlier this month, Donald Trump suggested using
“a solid flu vaccine … on corona”. Not possible, scientists informed him. When
he declared that a vaccine would be available within a few months, he had to be
told that, in that time, vaccines would only be ready for testing. Ordinarily,
human trials come after many phases of animal testing, but at least two
companies – one of them Moderna – have decided to do both in parallel. The scientists
I spoke to, though, kept telling me that testing couldn’t be rushed. “There
will be many trials, and we need to be ready for some failures,” Heeney said.
He leaned in towards his webcam as if to push his point physically through the
internet to me. “We have to avoid overpromising, because if there’s an accident
with one of those first vaccines – if someone gets ill and it gets into the
Daily Mail, ‘New vaccine threatens survival’ or some ridiculous headline – then
people won’t want to take even the later vaccines that do work. It’s a razor’s
edge we’re walking here.”
{kind=link}
Comments
Post a Comment